
Insights
Private delivery, public purpose: getting the balance right in Australian healthcare
02/03/2026
Australia’s health system is routinely described as “mixed” – a blend of public and private. That is true, but it often sends debate down the wrong track. The central policy question is not ownership for its own sake. It is whether incentives, information and accountability are aligned so that whoever delivers care does so in the public interest.
Private organisations already deliver a substantial share of care across Australia – hospitals, diagnostics, community services, and a growing range of digitally enabled models. In practical terms, the task is to capture the upside private delivery can bring (innovation, responsiveness, operational performance and, in some case, additional capacity) while managing predictable risks: variable quality, inequitable access, cost escalation, fragmentation, and opaque ownership in services that patients and governments cannot simply “walk away” from.
If reforms are to endure beyond electoral cycles, Australia needs a clearer organising framework – one that separates questions of payment from questions of delivery, and then tightens accountability where the public interest exposure is greatest.
Start with the distinction that matters: who pays vs who delivers
A useful starting point is to separate who pays from who delivers. A simple 2x2 covers most of what matters in practice:
Figure 1 Healthcare Payment & Delivery |
|
Source: ACIL Allen |
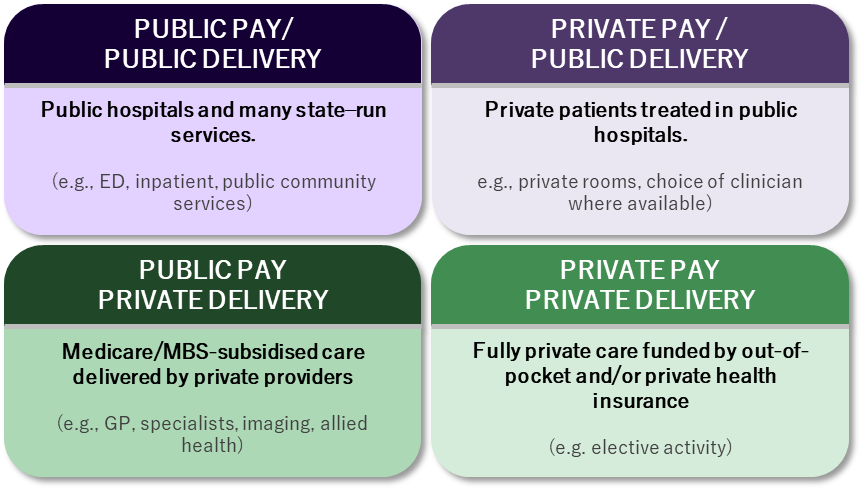
This distinction matters because the risks and remedies differ by quadrant. Concerns about “privatisation” often conflate privately funded care with privately delivered care funded by taxpayers. Yet the policy levers that protect equity and value – pricing rules, access settings, outcomes transparency, safety oversight and competition policy – depend on which quadrant is under discussion.
Australia’s challenge is not whether private organisations exist in the system. They do. The challenge is whether our operating settings are modern enough for a mixed model under contemporary pressures.
Where private delivery can add value
Private delivery is not inherently superior or inferior to public delivery. Performance depends on incentives, information, market structure and accountability. That said, there are settings where private providers can create system value when governance is fit for purpose.
Innovation and pace of change
In parts of the system – particularly diagnostics and some digitally enabled models – private providers can adopt and scale new tools and workflows quickly. That can benefit patients, but only if innovation is paired with evidence, safety assurance and interoperability. Proprietary fragmentation is not innovation; it is a future integration bill.
Operational performance in high-volume pathways
In repeatable, high-throughput services (for example day procedures and some elective streams), private providers may bring strong scheduling discipline, procurement capability and process improvement. This can lift throughput and relieve pressure where capacity is constrained. The public value, however, depends on price and quality settings being explicit; otherwise volume incentives dominate, and costs rise without commensurate outcome gains.
Specialisation and capital-intensive capability
Some services require concentrated expertise, specialised infrastructure and sufficient volume to maintain quality. Private providers can help build and sustain that capability and, in some cases, mobilise capital for facilities and technology. As clinical complexity rises, however, transaction costs rise too: coordination, information sharing and continuity across general practice, hospitals and community care become non-negotiable conditions – not optional aspirations.
Flexibility and surge capacity – within a system workforce constraint
A mixed ecosystem can improve resilience by providing extra capacity where demand surges or workforce availability is uneven. But in a constrained labour market, “new capacity” can also be workforce reallocation. Private expansion that draws staff from essential public services can worsen system performance overall unless workforce planning is managed at a system level.
Private delivery can be an asset. It is not self-justifying. It should be used against clearly defined outcomes – and held to those outcomes.
The downside risks are predictable (and manageable)
The risks associated with private delivery are well-described internationally and familiar domestically. They tend to show up in five places:
- Safety and quality variability when service growth outpaces governance capacity, data transparency and consistent standards.
- Equity and access pressures when gap fees, geography and service availability create de facto two-tier access.
- Cost escalation when incentives reward volume over value, and when prices and performance are not transparent to patients or funders.
- Fragmentation where care crosses organisational boundaries – public / private interfaces, hospital-community transitions and multi-provider pathways.
- Workforce displacement when cross-sector competition for staff is unmanaged.
None of this requires an ideological conclusion. It requires governance that follows the patient rather than the institution, and contracting arrangements and operating settings that recognise information asymmetry and thin local markets.
One system, split responsibilities: Australia’s federal constraint
Australia’s institutional design adds a structural complication: Commonwealth funding levers sit alongside state and territory responsibilities for much of delivery. The result is a persistent tension – particularly when one level of government bears the operational consequences of incentives set elsewhere.
Two national pillars have helped hold the system together:
- Medicare, which provides a nationally consistent platform for subsidised out-of-hospital care; and
- the National Health Reform Agreement (NHRA), which underpins public hospital funding and shared reform intent.
These settlements were built for an earlier operating environment – more focused on hospital expansion and episodic acute care. The system now faces different pressures: chronic disease complexity, workforce constraints, rapid population growth, rising expectations, cyber risk, and technology-driven change (including AI). Updating intergovernmental settings is not “reform theatre”; it is routine system upkeep in a mixed model that is operating under new stressors.
Profit, ownership and essential services: tighten accountability where switching is hard
Profit is not inherently incompatible with public purpose. Many essential services are delivered by organisations with commercial objectives. The policy question is whether incentives and accountability are strong enough in essential services, where switching costs are high, local markets can be thin, and continuity is a public necessity.
This is where complex / financial investor ownership warrants explicit, non-partisan attention. The risk is not “private capital” in the abstract. It is the interaction between service essentiality and structural features that can amplify fragility or opacity, including:
- shorter investment horizons relative to long-term stewardship needs
- higher leverage and refinancing risk, reducing resilience to shocks
- related-party arrangements (property, management fees, service contracts) that can obscure true cost and performance
- incentives to optimise financial returns ahead of quality, workforce development or continuity unless obligations are explicit and enforceable
The policy response should be proportional: the more essential the service and the thinner the market, the higher the transparency and continuity expectations should be.
Practical principles that fit the problem:
- Ownership disclosure for essential service providers, including ultimate beneficial ownership and material related-party arrangements.
- Financial resilience expectations calibrated to service risk, including stress testing against demand, cyber and workforce shocks.
- Continuity-of-service obligations, backed by credible contingency planning.
- Comparable outcomes reporting across sectors, so performance is visible and contestable.
- Price transparency where patients and funders face material information asymmetry.
These settings are not novel. They mirror how governments manage risk in other forms of essential infrastructure.
Making the mixed model work: minimum conditions and enabling infrastructure
Because private delivery is an established feature of Australia’s system – and is likely to remain so – reform should focus on two things: (1) minimum conditions that force alignment with public purpose, and (2) enabling infrastructure that makes those conditions enforceable in practice.
Minimum conditions
- Outcomes accountability that follows the patient. Public reporting on safety, outcomes and experience across both public and private delivery. If measurement is not consistent, management will not be consistent either.
- Risk-based safety oversight. Assurance and incident learning that keep pace with service growth, focused where harm risk is highest.
- Funding that rewards value. Payment settings that support appropriate care, continuity and outcomes – not just activity.
- Market power management. In concentrated markets, rely less on assumed contestability and more on explicit obligations, transparency and – where necessary – regulated expectations.
- System-wide workforce strategy. Training pipeline, scope optimisation, supervision capacity and cross-sector planning that treats workforce as a shared national constraint.
- Interface governance. Shared pathways, information standards and clarity of responsibility at the points where failure is most common: primary care–hospital transitions, discharge, and multi-provider pathways.
Enabling infrastructure
- Interoperable digital foundations that support continuity and outcomes measurement across organisational boundaries.
- Cyber security treated as a patient safety prerequisite, with minimum controls and mature incident response across the supply chain.
- Workforce development aligned to future models of care, including placements and credentialing that support mobility without destabilising essential services.
- Governance capability that keeps pace with new technologies, ownership models and cross-sector delivery.
- investment settings that steer capital toward productivity-enhancing modernisation, not simply activity growth.
A practical test for the next phase of reform
Australia does not need to choose between “public” and “private” as if a label guarantees good outcomes. It needs clarity about what it is trying to optimise: access, safety, quality, value and sustainability.
Private delivery can contribute materially to those objectives – provided public interests take precedence over private incentives in essential services. That means modernising the operating settings beneath the mixed model: strengthening transparency and assurance, improving intergovernmental coherence, investing in digital and cyber foundations, and treating workforce as a national constraint to be managed across sectors.
A simple test is also the most useful:
Does this arrangement improve access and outcomes safely – and can we demonstrate that with transparent data?
If yes, the system should be confident in using the strengths of both sectors. If no, the answer should not be a slogan. It should be redesign.